3D Printing an Obturator for an Immediate Load AllonX Case
Patients who come into the dental office needing full arch rehabilitation are unique and thus each and every patient needs to be evaluated uniquely for how to approach their particular treatment. So many times clinicians reach out to me asking “how do you treat your AllonX cases?” While this is a great question for sure and a topic that I cover extensively in our online course (www.LearnAllonX.com), the main key takeaway of every lecture on the topic I give is that we must treat each patient individually and uniquely. I recently had a patient seek my office because of the unique approach we take to digital dentistry.
A patient requested an appointment to discuss full arch rehabilitation. As part of my recommended exam protocol, the patient began with my dental assistant – facilitator who started the record gathering procedure. Radiographs, essential charting, and extraoral and intraoral photographs were made.


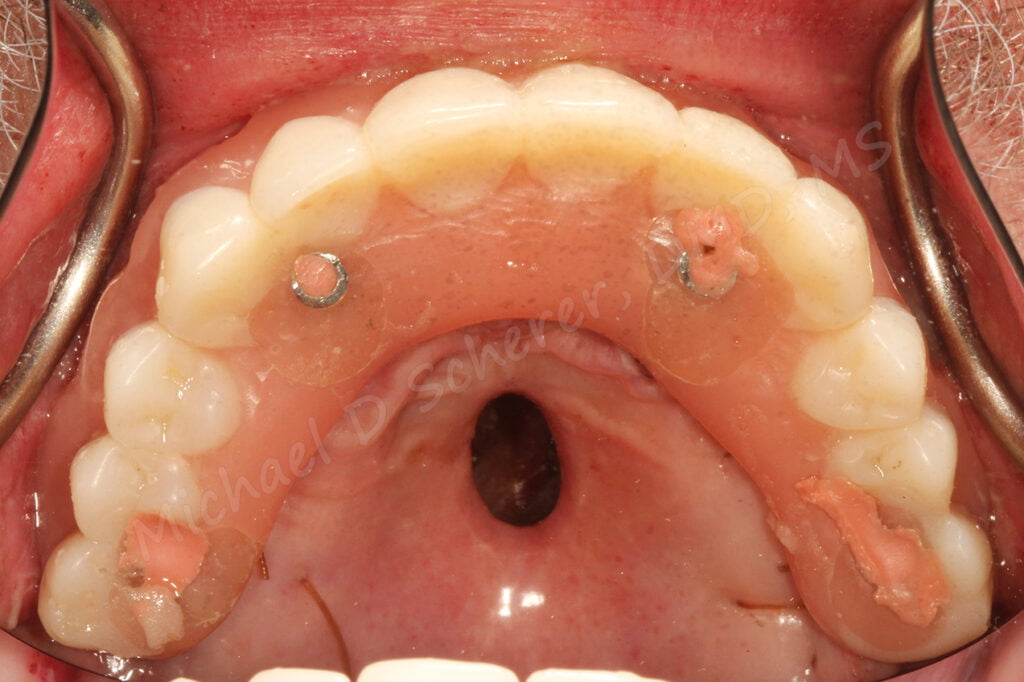
My assistant saw the patient was wearing a removable partial denture so she asked the patient to remove it and she noticed that it was filling a gap in the patient’s upper portion of his palate.

The patient was successfully wearing an RPD that was filling, or obturating, a mid-palatal defect. The hole connects his oral cavity to his nasal cavity! How this happens is due to a variety of reasons including: oral cancer, trauma, birth defects, and more. It can be closed with surgical revision, however, in this patient’s case, multiple surgical revisions were attempted and this closure was the best we could get. In fact, he doesn’t have much hard palate at all – most of the palataine process of the maxillary arch was missing!
His main concern was given early in the appointment. He said, “Doctor, I know I need an implant bridge but I have seen other dentists who said they couldn’t do it and plug the hole in the top of my mouth at the same time!” I looked at the patient and understood why… if we were going to do an immediate load AllonX prosthesis, there are so many variables to contend with, especially since his case was a challenge from a surgical perspective as well!
His case was was a challenging case for my surgeon and I. Thankfully he had plenty of alveolar ridge Zone I bone, but he had little to no Zone II and III bone! We worked up the case together and determined that was possible was was placing two implants in Zone I and two zygoma implants in Zone III. Surgically, this is a very reasonable plan and a type of AllonX procedures we do often, but the biggest challenge was managing his prosthetic goal – immediate sealing, aka obturation, of his palatal defect with a device attached to his interim AllonX prosthesis.
To accomplish his goal, I made intraoral scans using a 3Shape TRIOS scanner with and without his RPD in place to help guide my prosthetic position of teeth and the obturator.




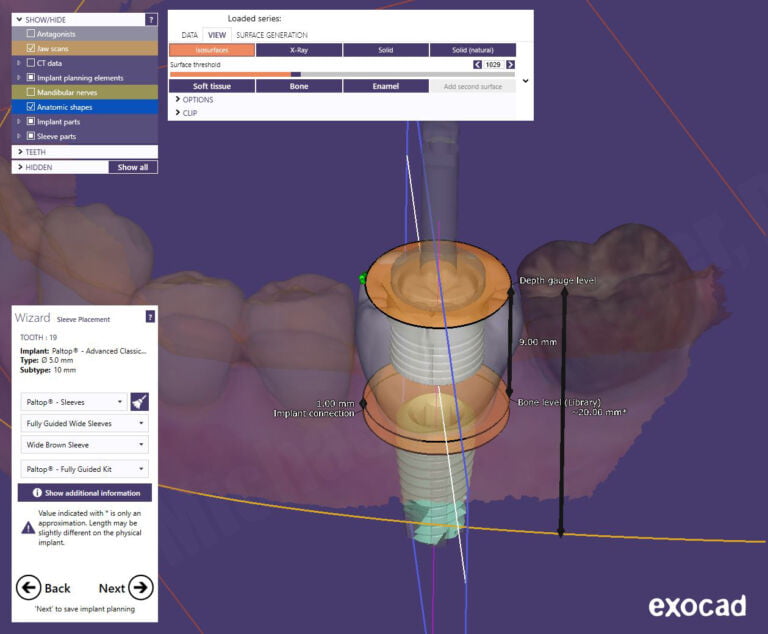
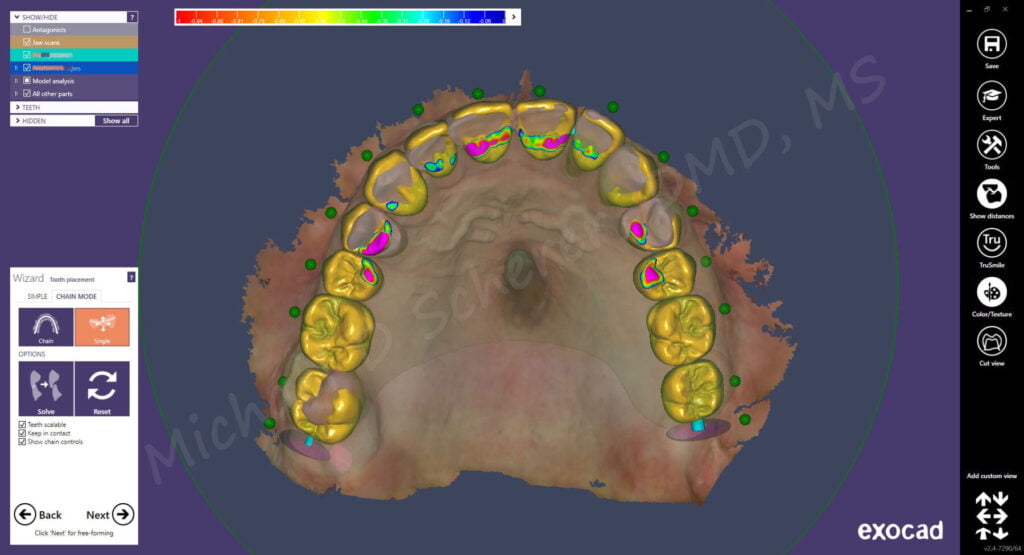
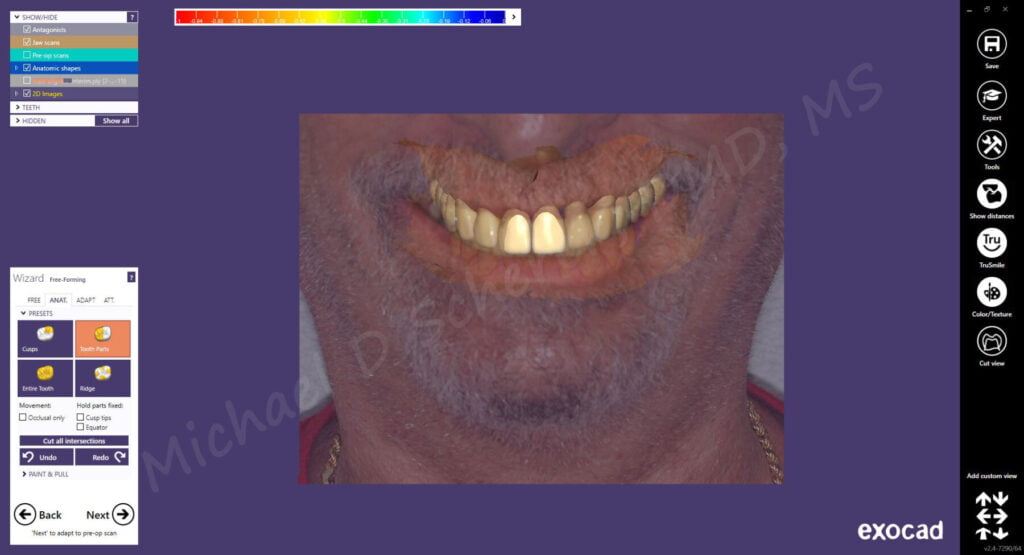
I imported the scans into exocad design software for designing an immediate denture that I could mill or print to use immediately after surgical procedures to convert into an immediate load prosthesis. Using the software, I could import his intraoral scans, overlay both the existing RPD prosthesis and his face scan to digitally design his immediate load AllonX prosthesis. I segmented out the teeth into 3 segments to allow me to easily mill and bond the parts into the milled base.
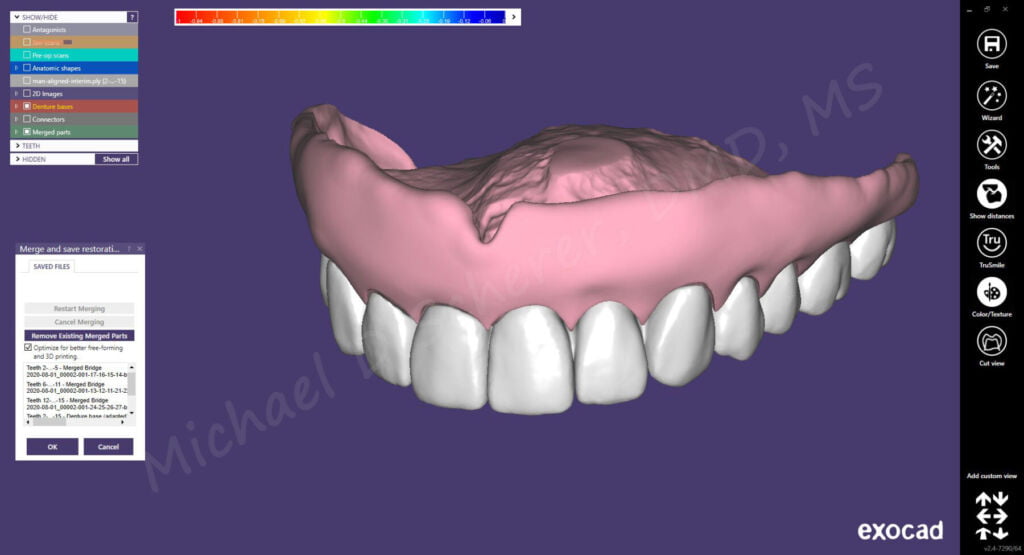
After designing the teeth and base of the prosthesis, I exported from exocad and imported into the CAM software of a VHF K5 mill. Using Ivoclar Ivotion discs, I milled the teeth using multi-layered tooth colored materials and the base using a pink base material. Using the bonding system from Ivoclar, my technician bonded the teeth to the base and finished the prosthesis.

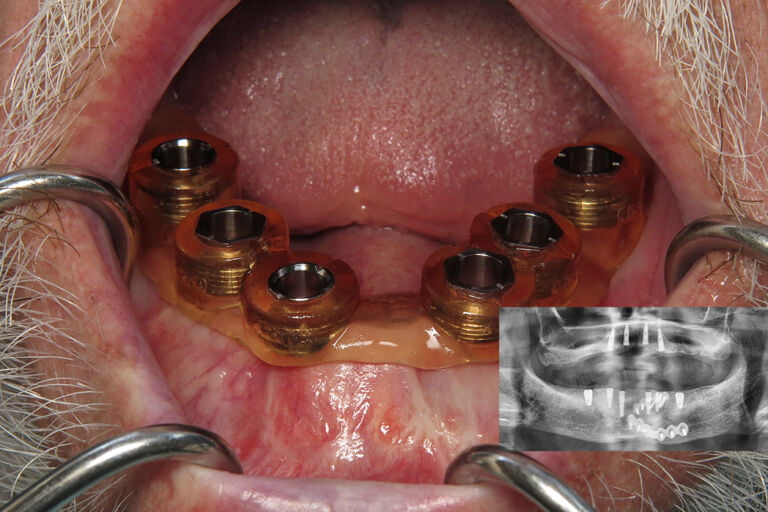
I met the patient at my surgeon’s office where his teeth were extracted and 4 Noris Medical implants were placed including two Zone I standard form implants and two Zone III zygoma implants. I placed multi-unit abutments and cylinders and prepared holes within the denture. Using Zest Dental Solutions CHAIRSIDE Attachment Processing Material (BTW: the best stuff on the planet for picking up cylinders for AllonX!!), I luted the cylinders to the milled prosthesis. After a bit of finishing, I placed the prosthesis onto the implants and thus completed the AllonX prosthesis conversion procedure.
Note: If you’re interested in learning about how to do the above steps, check out our AllonX online course (www.LearnAllonX.com)


While with most AllonX patients, my tasks would be done for the day at my surgeon’s office, however, this case was different. At this point, with the prosthesis placed, the goal is to scan the patient to make a same-day interim obturator. Sure I could have designed something super fancy with clasps or possibly vacuum formed with reline material in it, but I really wanted to exceed this patient’s expectation during his transition from natural teeth to AllonX with something super small & comfortable.
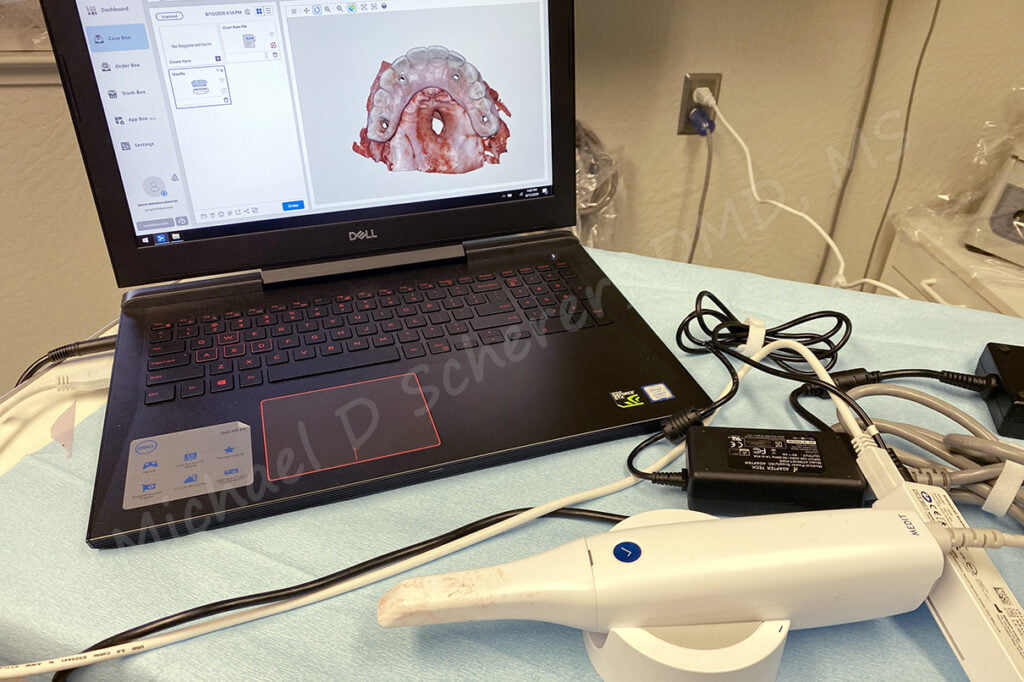
I decided to bring my Medit i500 scanner to my surgeon’s office since it’s very portable and easy to transport. I scanned the patient’s new immediate load AllonX prosthesis immediately after placing the prosthesis. I didn’t think I would need the opposing but I could have scanned the opposing as well; I chose not to for expediency sake.
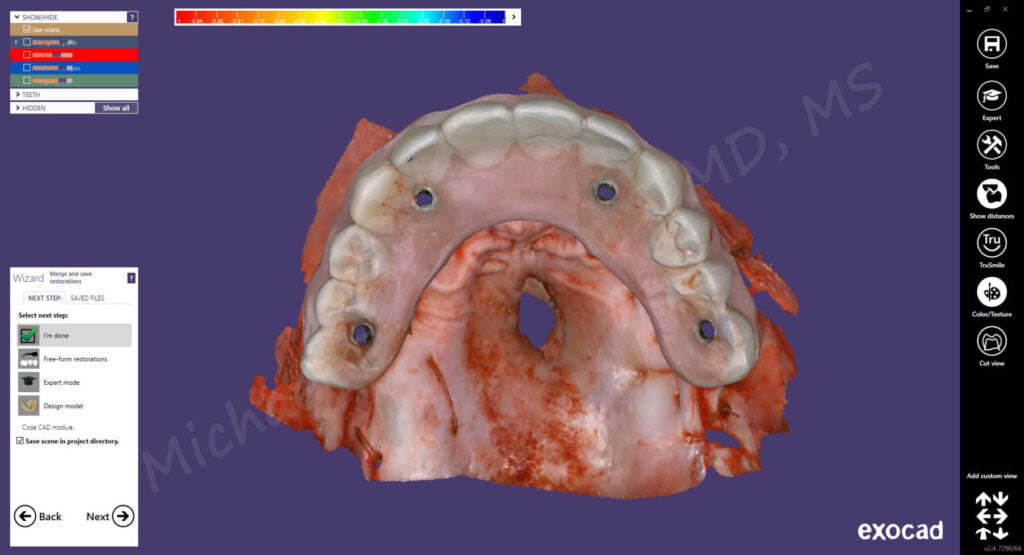
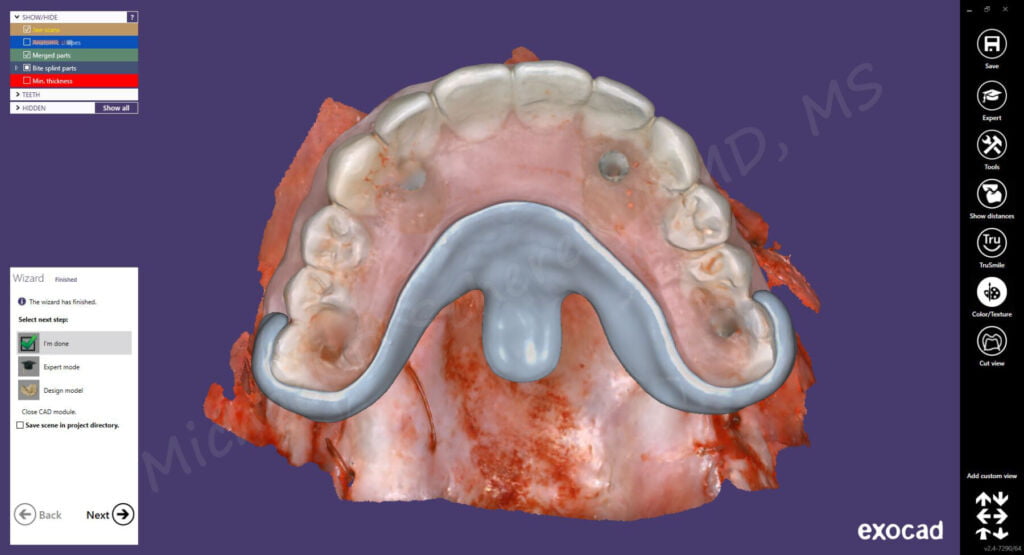
Since my Medit i500 is connected to exocad software, it was a matter of step-by-step wizard workflow to import the scans into exocad. I brought the scans in as a bite splint design where palatal defect undercuts were surveyed and blocked out and a special design was made around the AllonX prosthesis to allow for a clasping like effect. I didn’t want to have anything on the occlusal of the AllonX prosthesis since the patient was going to wear the obturator prosthesis during the daytime to assist with his speech.

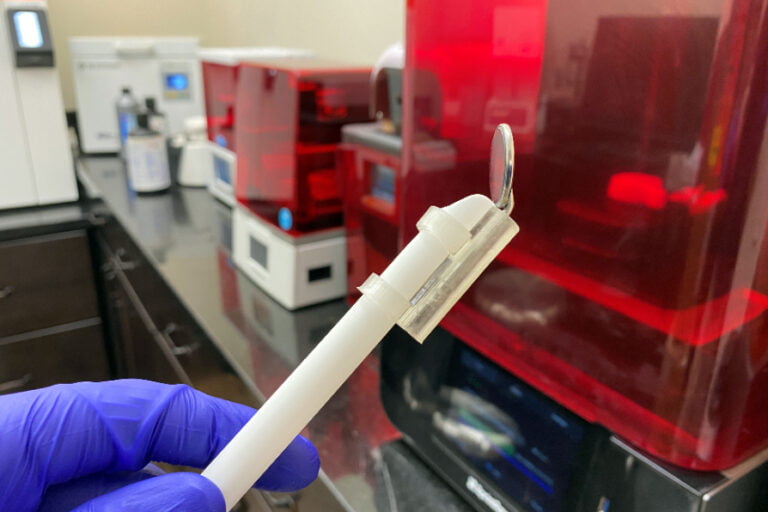
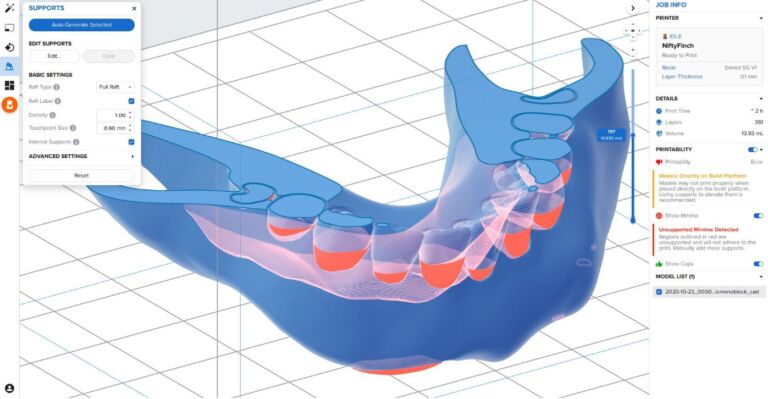
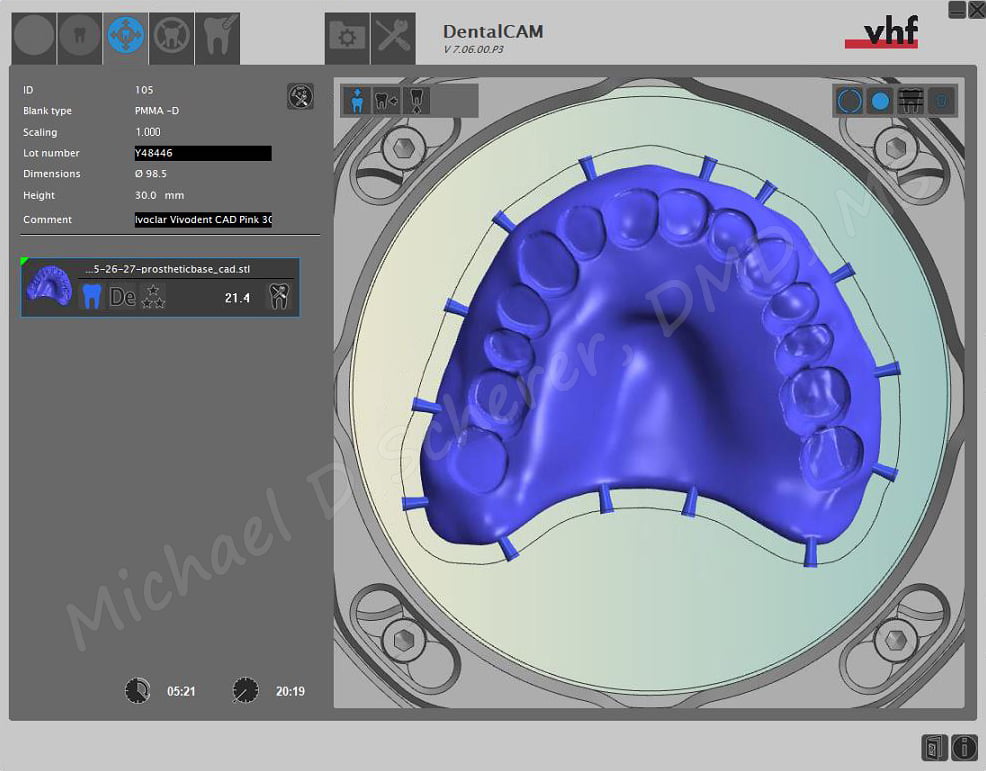
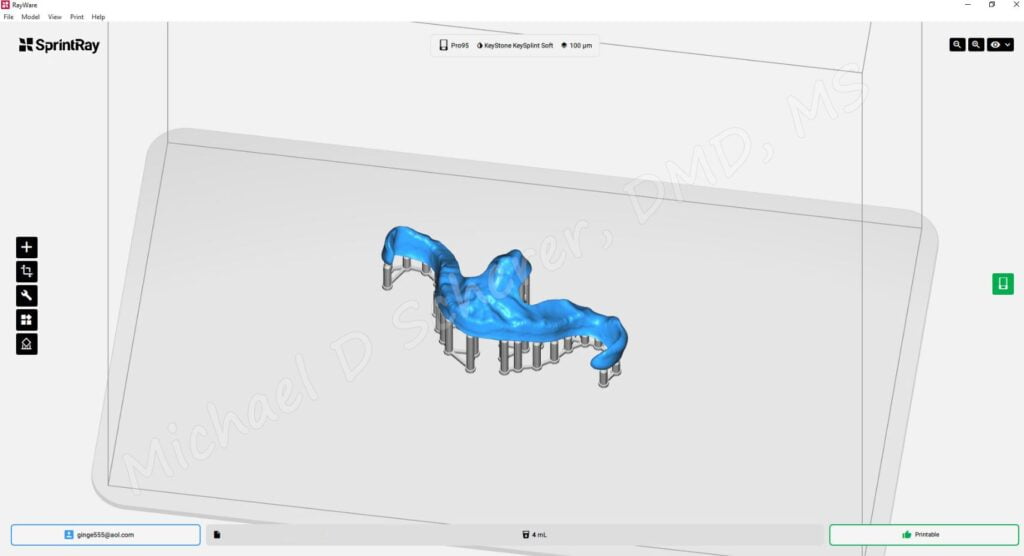
After designing the immediate obturator, I remotely connected to my lab computer and exported the designed file into Rayware software for preparing to print on a Sprintray Pro 3D printer. I decided to use Keystone KeySplint Soft for this prosthesis because I purposely could design a bit of undercut retention within the design to enhance the ability of the immediate obturator to engage undercuts without making it too difficult for the patient to remove. Ultimately an immediately loaded AllonX prosthesis shouldn’t have much torsional or torquing effect placed upon it, which a traditional wire clasp prosthesis could potentially impart. Yeah call me crazy but I think about these things.
I clicked print and 45 minutes later I would have a printed prosthesis. During this time the surgeon is bringing the patient out of sedation, performing routine post-operative procedures such as a panoramic radiograph and post-op instructions. Once the prosthesis was fully printed, I went to my office (a short drive away) and removed the build platform from the printer. I removed supports, polished, and UV cured the prosthesis.

I returned to my surgeon’s office and they were just finishing up the post-operative protocol and instructions. I placed the printed immediate obturator and the fit was great but just a tiny bit loose! KeySplint Soft allows the clinician to heat up the material and do a small amount of thermoforming chairside so I took a bowl of hot (not boiling) water and soaked the interim obturator for a minute. I replaced back around the AllonX prosthesis and gave it a bit of a squeeze around the clasps and allowed it to cool.


After allowing it to cool, I removed the prosthesis and re-inserted it. A perfect fit… I was blown away!

After revealing the patient’s new smile, I also showed him what we were able to accomplish with digital dentistry… tears came down his face. He was blown away also. With a wry smile, he said, “See Doc, I knew you could do it!” He smiled.
We both laughed and talked about home care and his next steps. I slept well knowing that we accomplished something special for our patient and I genuinely felt like we exceeded his expectations!

Online Course
Interested in learning more about Full-Arch Implantology? Want to learn how to do step-by-step AllonX implant planning, surgical and prosthetic steps, and digital protocols in your office and/or laboratory? Check out our innovative step-by-step online AllonX course at www.LearnAllonX.com

Dr. Michael Scherer, DMD, MS
Dr. Michael Scherer is an Assistant Clinical Professor at Loma Linda University, a Clinical Instructor at University of Nevada – Las Vegas. He is a fellow of the American College of Prosthodontists, has published articles, books, and in-person and online courses related to implant dentistry, clinical prosthodontics, and digital technology with a special emphasis on full-arch reconstruction.