Implant Overdentures: To Frame or Not To Frame? “That is The Question!”
I teach a lot of implant overdenture treatment and therapy. It’s not only a huge part of my practice, it’s a topic that I have extensively researched, published, and helped spread the word to clinicians around the world in both in-person and online.
One question I get almost universally is, “Doctor, do you put frameworks routinely in your overdenture cases?” That is a very good question that does take a bit of discussion! There are many variations of overdentures including those with bars and with standard LOCATOR cases. For simplicity sake for writing this article, let’s concentrate on the tissue-supported, implant retained, LOCATOR-style overdentures.
Some clinicians and technicians mention, “I routinely put in a framework into my overdentures, it strengthens it!” or “I only put in frameworks when the patient breaks starts breaking their denture!” There’s a fair amount of controversy for sure so I figured I would put together this article to openly have a discussion regarding the question: “To Frame or Not To Frame… that is the Question!”
I do not routinely place reinforcement frameworks within my overdentures unless the treatment falls into one of a few conditions.
Michael D Scherer, DMD, MS
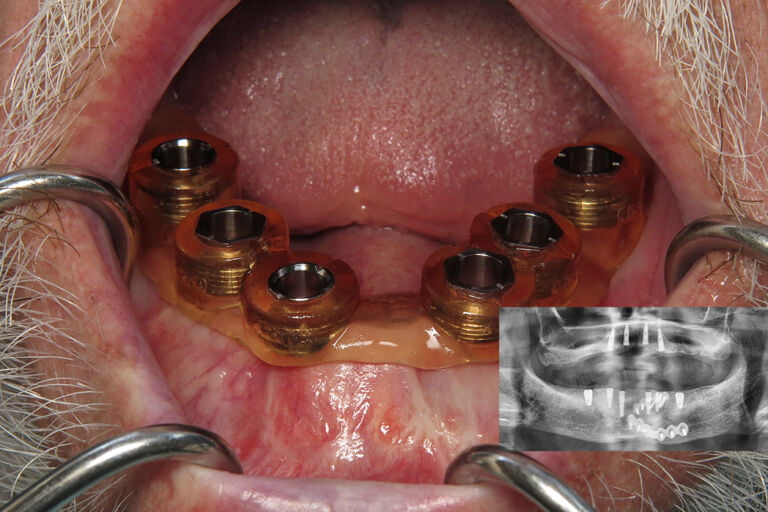
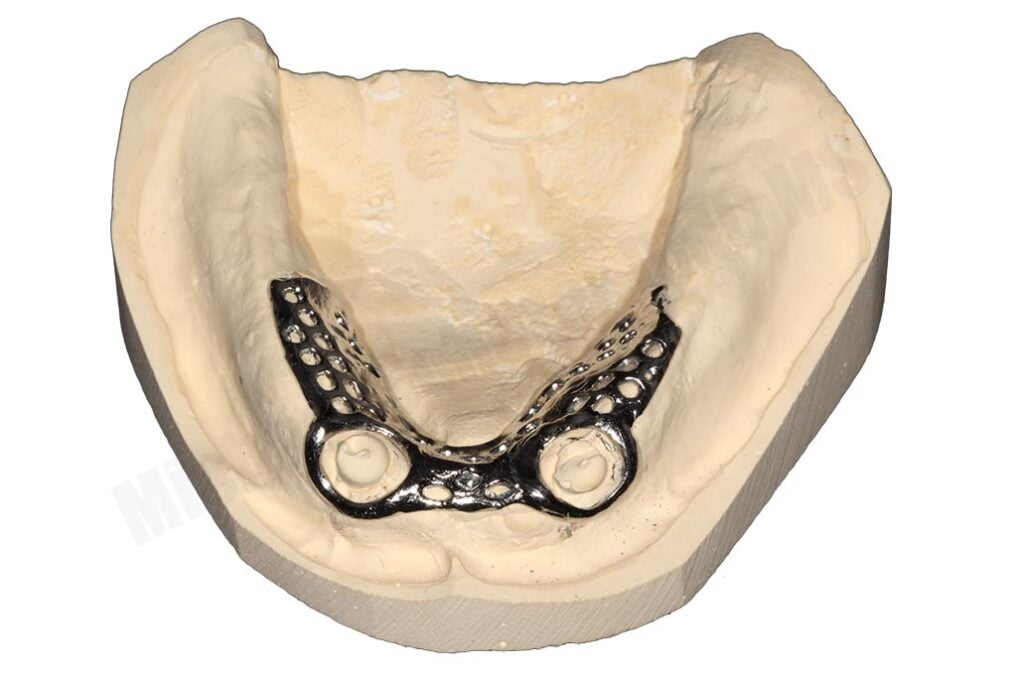
Let’s start with a clinical case example that helps clarify a clinical situation that is, unfortunately, quite common. A patient had existing overdenture treatment and a few months later started reporting fracture of his denture on a regular basis, approximately every two weeks. It became increasingly frustrating for the patient and we treated him successfully with revision treatment, including fabrication of his mandibular prosthesis with a framework in the processed acrylic.


While this clinical example also involved surgical revision therapy, a framework was indicated here (example shown later in this article) as the patient has had a history of fracture of the existing prosthesis due to bruxing forces and limited prosthetic space. Why did I choose a framework here versus other cases? What are some indications of when we would put in reinforcement mechanisms into an acrylic prosthesis?
Conditions that I typically recommend using retention frameworks with overdentures:
- Maxillary Arch & Patient Desire for “Palate-less Design”
- History of Bruxism
- Limited Interarch Space – aka “Prosthetic Space”
- Bar Overdenture Treatment (not covered in this article)
Restoring a patient with a palate-less maxillary overdentures is my #1 reason to use a framework reinforcement. The principle reason why is that the vast majority of patients who desire implant treatment for the maxillary arch and are interested in removable options typically have existing complete dentures and want to eliminate the palatal coverage. Additionally, those same patients like the open palate design which then decreases the amount of support the prosthesis has on the arch. With less prosthetic support, there is less bulk of the prosthesis and potentially increasing the risk of fracture of the prosthesis.


Patients that are bruxers are also susceptible to imparting a huge amount of stress on the acrylic of the overdenture. Bar overdentures are likely the most susceptible to patients who are bruxers as well as bar overdentures are typically more implant supported than implant retained. As a result, patients have little negative feedback loop (nociceptive reflexes) for them to resist the grinding forces against their prosthesis.



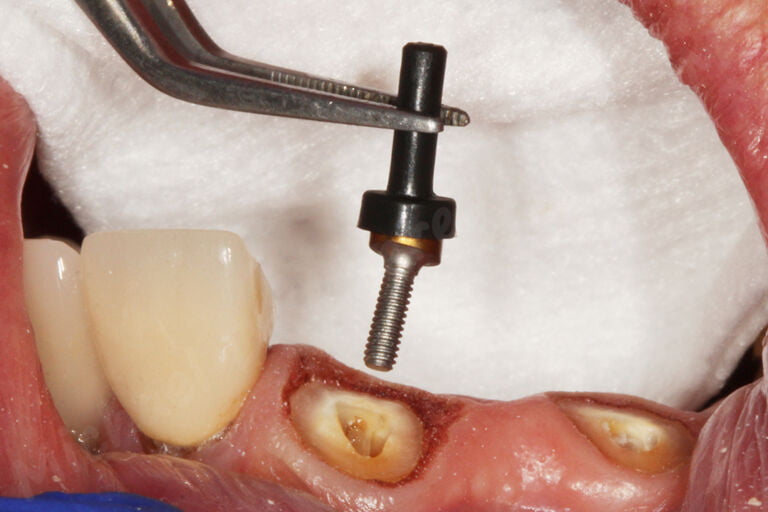
To properly treat a patient with LOCATOR or most stud-style overdenture abutments, most experts recommend 9-11mm of prosthetic room from the top of the implant to the outside (or cameo) surface of the denture. If a denture has less than that recommended thickness, fracture of the prosthesis can occur. When limited prosthetic space exists, many advocate for using a metal re-inforcement framework to help keep the denture from fracturing.

While there is much controversy surrounding this very important topic, I do not routinely place reinforcement frameworks within my overdentures unless the treatment falls into one of a few conditions mentioned previous in this article. Routinely adding a framework into an overdenture prosthesis doesn’t hurt and I do support clinicians technicians who just feel strongly that it should be routine treatment. I do caution you and those reading this article that routinely adding frameworks increases laboratory costs, bulkiness of the prosthesis, weight of the prosthesis, complexity of fabrication process, and potentially more challenging relining procedures when indicated.
The key is being open to knowing that what we as clinicians, technicians, and team members do is we must be cautious with the “same size fits all approach” – meaning treating everyone with the same treatment. We should know when to adapt our philosophies. We must be open to alternative ideas and know when to use some techniques over others. When we learn together, we grow together!
Want to learn more about full arch implant dentistry and implant overdentures? Make sure you check out our online course Fast Track Full Arch Dentistry – Implant Overdentures with 11hr of CEU by UNLV School of Dental Medicine. Visit www.LearnOverdentures.com

Dr. Michael Scherer, DMD, MS
Dr. Michael Scherer is an Assistant Clinical Professor at Loma Linda University, a Clinical Instructor at University of Nevada – Las Vegas. He is a fellow of the American College of Prosthodontists, has published articles, books, and in-person and online courses related to implant dentistry, clinical prosthodontics, and digital technology with a special emphasis on full-arch reconstruction.