Root Resurgence – LOCATOR Root is Back!
A seemingly long time ago [in a galaxy far, far away], the rage in dentistry was the use of special attachments cemented into residual roots to help retain and support an denture or partial. It was an exciting time, a pioneering time, and one that we have seemingly forgotten about in our dental implant world.


Some even went as far as claiming the 1970’s was the decade of the overdenture and this mentality has even reached the scientific literature. It makes sense, why would that time period be so important for overdentures? Before the Toronto conference in the early 1980’s, many clinicians looked at dental implants seemingly as voodoo magic or for those wild-crazy experimental people. Complete tooth loss was a significant part of everyday life, who knows, maybe there was just a bit too much fondue and twinkie consumption at the time (lol). Joking aside, dentists had to figure out how to avoid the dreaded tissue-supported complete denture and noticed that some teeth, maxillary and mandibular canines especially, were strong enough to use as attachments to hold a denture into place.
Fast forward to today, treating edentulous patients is a relatively routine part of many of our clinical practices. We are comfortable with the 2-implant LOCATOR overdenture and many of us think that the mandibular overdenture treatment is implants or just a standard denture. Let’s stop right there – I propose a middle ground!! Many of us are comfortable with endodontic procedures on anterior teeth including maxillary and mandibular canines. Why not combine two amazing parts of dentistry?
I often see the limitations to patient acceptance of implant treatment is often the expensive cost of the procedure and fear of surgical procedures to have implants placed. Certainly both of these factors can be accounted for and managed with many patients, I do find it a bit easier to get some patients to accept the idea of saving a few teeth to help stabilize their denture. The neat part is that it can be done immediately, the same day the teeth are extracted, so patients can have instant retention/stability of their prosthesis the day they get it! On top of the aforementioned, dental plans often have much better coverage for things like endodontic procedures and posts over dental implants and abutments. A surgical and cost savings can potentially get more patients to say yes more often to full-arch treatment! The key is figuring out how to make an denture or partial plus attachments as simple as possible.
Many of us are very comfortable with using LOCATOR abutments for implant overdentures and wonder “Do I have to learn something new to do these root cases?” No need to worry, it turns out that Zest Dental Solutions makes a LOCATOR for residual roots for this exact purpose! They even make 3 different angle options for cases where root structure is divergent to ensure that parallelism is in line with the path of placement of the prosthesis. Wow!!

The general idea is an endodontically treated dental root is prepared like a stainless steel or cast post and instead of cementing in a post for retaining a core for a crown procedure, one would simply cement a post with a LOCATOR abutment sitting on top. The tooth root would remain and the superior portion of the post would have a standard LOCATOR abutment, which is functionally and mechanically identically as one that is on a dental implant. Housings, nylon inserts, and any parts are fully interchangeable and compatible with the implant version of LOCATOR. Cool!!!!

Ok so it sounds interesting, but what are some key indications for using LOCATOR Root?

From what I have seen in my practice, LOCATOR Root fits as a really important part of treating patients. Maybe it’s because a big part of my practice is older patients, but typically I see the biggest reason for using a root attachment is when a patient comes in with an existing removable partial denture and a key abutment tooth has fractured. Typically these patients are older, with fairly significant medical comorbidity, and need to be cautious with their medical/dental costs as they are on fixed incomes.
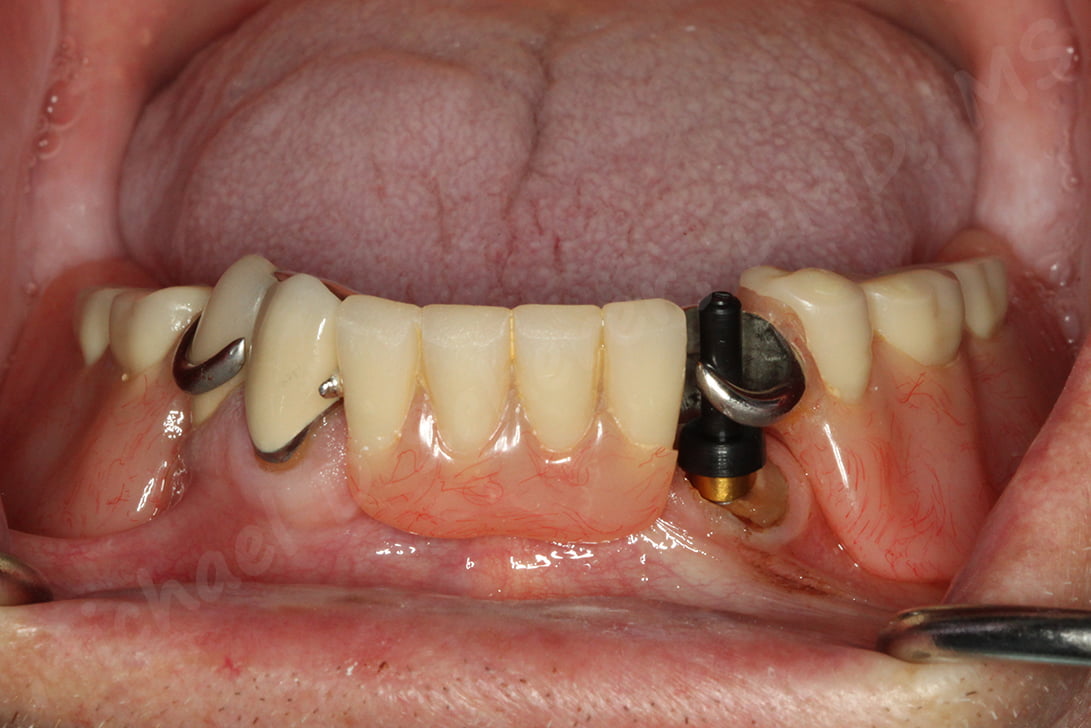
A patient presented with an existing mandibular removable partial denture with distal extensions and abutment teeth on #22, 27, 28. The patient indicated #22 fractured the existing crown on #22 and was worried that this would “mess up the partial” and would need a new one. While I went over other options including a new post/core and crown or an implant, he really loved the idea of placing a LOCATOR abutment into #22 and the immediate fix.

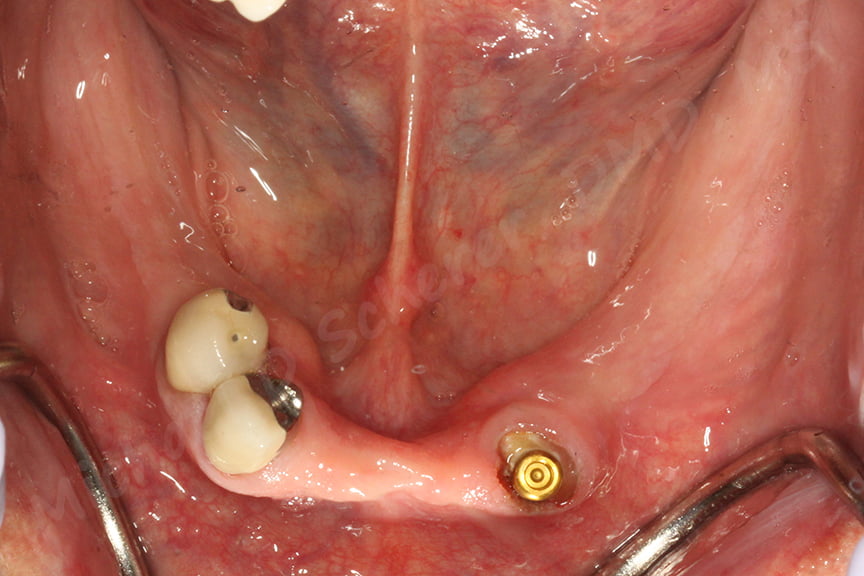
Since tooth #22 already had endodontic treatment, it was an ideal candidate for LOCATOR Root treatment. I prepared the root with the included drill and sized the LOCATOR Root abutment, verifying angulation by placing the abutment in with a Parallel Post carrier. This little carrier is ideal for confirming angulation of the path of placement of the partial or overdenture. By using this tool, one can see the proposed angulation of the abutment in relation to the partial surface.


Once confirming the full adaptation of the components with an x-ray, I cemented the post with a resin luting agent, CEM-EZ.


After cleaning up any excess cement, a Block-Out Space and Housing are placed on top of the abutment. The Housing is picked-up using Chairside Attachment Processing Material and any excess resin is polished away. The partial is taken to our laboratory area where a denture tooth is attached to the existing partial denture.


The patient is shown how to insert and remove their newly fitting partial denture including how to care care of the inserts and retention elements. He was successfully treated in a single visit in approximately 1 hour of total treatment time including the laboratory procedures to attach a tooth. The patient was blown away… instead of multiple visits and huge expenses, he walked out with a cost-effective solution in the same appointment!!
Want to learn more about full arch implant dentistry and implant overdentures? Want to find out more step-by-step clinical protocols and techniques? Make sure you check out our online course Fast Track Full Arch Dentistry – Implant Overdentures with 11hr of CEU by UNLV School of Dental Medicine. Visit www.LearnOverdentures.com

Dr. Michael Scherer, DMD, MS
Dr. Michael Scherer is an Assistant Clinical Professor at Loma Linda University, a Clinical Instructor at University of Nevada – Las Vegas. He is a fellow of the American College of Prosthodontists, has published articles, books, and in-person and online courses related to implant dentistry, clinical prosthodontics, and digital technology with a special emphasis on full-arch reconstruction.